Da Nang, Vietnam – late 1976.
The influenza arrived without warning, sweeping through the city’s overcrowded nursing homes like fire through dry grass. It was a brutal strain: high fever, violent coughing, and lungs that filled with fluid faster than the body could clear them. In a country still reeling from war, hospitals were shells of buildings, ventilators did not exist, oxygen cylinders were rarer than gold, and antiviral drugs were a fantasy.
At most facilities, the elderly began dying within hours of the first cough. Mortality rates climbed past 40%, sometimes 60%. Bodies were carried out under mosquito-net shrouds while the living waited their turn.
But at one small state-run home on the outskirts of the city (today remembered only as Nhà Dưỡng Lão Số 3), something different happened.
Not one resident died. Not a single one.
The director, Dr. Nguyễn Thị Minh, was 34 years old and had trained as a battlefield nurse. She had seen lungs drown in blood and mud; she knew what drowning looked like. When the first cases appeared, she gathered her staff (mostly teenage volunteers and grandmothers who had lost their own children to the war) and told them the truth: “We have no machines. We have no medicine. We only have our hands and time. So we will use both.”
They cleared the dining hall and turned it into a ward. Every bed, every mat, every door laid flat on bricks became a treatment surface. Then came the idea so simple it sounded absurd.
Towels.
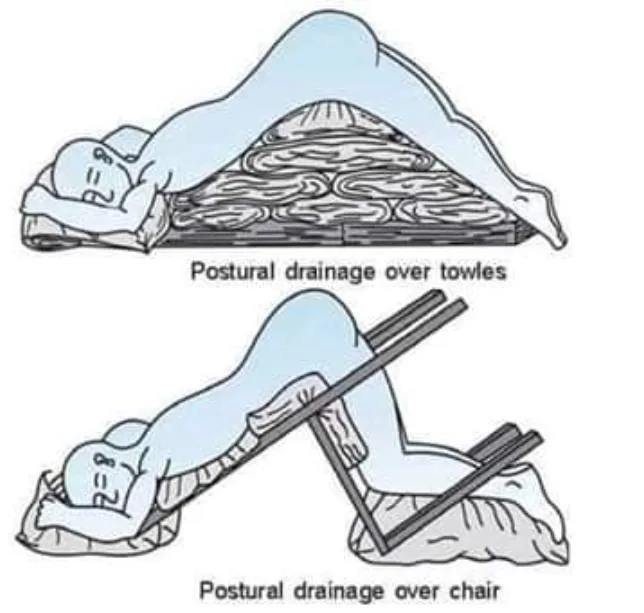
Thick cotton towels, folded and rolled, were placed under each patient’s pelvis or chest so the head and shoulders hung lower than the hips. Stretchers were tilted ten, maybe fifteen degrees (just enough for gravity to do what medicine could not). Every twenty minutes, a caregiver gently clapped the patient’s back and sides with cupped hands: postural drainage and percussion, techniques borrowed from treating war-related lung injuries and childhood diphtheria.
When someone grew too weak to cough, a volunteer lay beside them, pressing rhythmically on the chest to force air out and bring mucus up. They worked in shifts of four hours on, four hours off, singing lullabies, wiping brows, whispering “Cố lên bà, cố lên ông” (“Hold on, grandma, hold on, grandpa”) until their voices cracked.
They boiled lemongrass and ginger on wood fires because it was all they had for fever. They rationed the single thermometer. They kept the windows open so the sea breeze could move through the room, carrying away the sick-air.
Night after night, the sound in that ward was not the rattle of death but the steady rhythm of hands on backs, the soft thump-thump-thump that said: we are still here, and so are you.
By the time the outbreak burned itself out two weeks later, surrounding homes had lost dozens of elders each. Nhà Dưỡng Lão Số 3 recorded zero deaths among its 87 residents (many of whom were over eighty and frail even before the flu arrived).
Word spread slowly, carried by exhausted doctors cycling between facilities. When a Ministry of Health inspector finally arrived, he found the patients sitting up, sipping rice porridge, asking for extra fish because they suddenly had appetites again.
He asked Dr. Minh to explain the miracle.
She held up a folded towel, still damp from the morning’s work.
“This,” she said, “is our ventilator.”
The story never made international headlines. No journalists parachuted in. The war had ended only a year earlier; the world had moved on. Even inside Vietnam, the details stayed quiet (partly modesty, partly because survival was so common it rarely felt like news).
But among generations of Vietnamese nurses and doctors, “the towel ward of ’76” became legend. Decades later, when young residents asked why we still teach postural drainage even in the age of ICUs and ECMO, the old professors would answer the same way:
“Because once upon a time, in a city with nothing, a handful of women and some folded towels were stronger than the virus.”
Sometimes the greatest medical breakthrough isn’t discovered in a laboratory.
Sometimes it’s remembered in the shape of a rolled-up piece of cloth and the sound of cupped hands keeping someone alive until morning.
Also Read this: The fight against flu viruses – archive, 1976
27 March 1976: The variability of flu viruses is frustrating for vaccine manufacturers, who have a constant struggle to keep up with the new varieties

Most encounters between man and microbe are of an intermediate sort. A flu virus arrives which is related to one that was around three years ago, and to which a proportion of the population has partial immunity. The upshot of this situation is very difficult to prophecy. Among other factors, it will depend upon the virulence of the virus, the ease with which it is transmitted from person to person, and the strength of the immunity in the human population.
In spite of these uncertainties, however, there are some very clear general guidelines. Waves of influenza A come to plague us roughly every two or three years, and outbreaks vary from a few isolated cases to epidemics that quickly involve 10 per cent or more of the population. Influenza B, which travels less quickly though the community, causes epidemics every three to six years.
Asian flu was a typical example of a new virus (labelled A) against which most of us were defenceless. Although the illness was generally mild, there were about 80 million cases of Asian flu. It spread at a remarkable rate and soon became disseminated widely throughout the world after originating in China in the spring of 1957. Within six months, there was a pandemic – a world-wide epidemic. Major changes of this sort in influenza A viruses occur about every 10 years, and the next such pandemic was that of Hong Kong flu in 1968.
In modern times, of course, air travel greatly facilitates such transmission. The earlier, catastrophic pandemic of 1918-19 moved rather more slowly, though its eventual toll was about a billion people – roughly half of the world’s entire population. Twenty million people died as a result of the 1918-19 pandemic, some as a result of pneumonia caused by the virus itself, some following secondary complications produced by bacteria.
There is no cross-protection whatever between A and B viruses; immunity against either type confers no resistance against the other. Within each group, however, there is some cross-protection. Antibodies formed in response to infection against one A strain, for example can afford some resistance against a related A strain. It is, of course, only during sizeable epidemics that the medical authorities usually have a detailed picture of which viruses are circulating and causing trouble. Indeed, many of the vague illnesses that we tend to label as flu may well not be influenza at all, but respiratory infections caused by other viruses and bacteria.
The variability of flu viruses is frustrating for vaccine manufacturers, who have a constant struggle to keep up with the new varieties. A vaccine that was highly satisfactory in conferring immunity against an epidemic strain last year may have little or or no value in forestalling the ravages of this year’s major villain. It is very difficult to isolate a new virus, in the Far East, say, and use it to produce a vaccine quickly enough and in sufficient quantities to immunise those who want or need it by the time the epidemic wave arrives in Britain.
All manufacturers can do is to ensure that their vaccines contain ingredients effective against most of the recently circulating strains. Attempts are, however, now being made to exploit those same processes of periodic change which flu viruses undergo in nature, to tailor-make potent vaccines more rapidly when novel variants do arise.
This season in Britain, we have seen moderate epidemics, particularly in London and the South-east, caused by two different A viruses (one of which originated in New Guinea last November) and by a B virus that appears to have caused more intestinal upsets than is usual with flu. Very recently too, microbiologists have become greatly concerned about the re-emergence, among young soldiers at Fort Dix, New Jersey, of an A strain closely related to, if not identical with, the one responsible for the 1918-9 pandemic. It seems that this virus, which is also virtually indistinguishable from that which produces swine influenza, may have been maintained ever since in pigs, until being transferred once again to humans.
What we do know is that antibodies against this virus can be found only in the blood of people old enough to have been infected in 1918-9. For the moment, the hopes are that because we are better nourished and because we now have antibodies to cope with bacterial complications, any epidemic triggered by this virus would be nothing like as severe as the earlier pandemic. But, as we have seen, predicting the ravages of flu is fraught with uncertainty.